

Smallpox is the only human disease that has ever been completely eradicated through a worldwide vaccination strategy. While we'd all like to believe that the Covid-19 vaccine will normalise society, the reality is a bit more moderate: mortality and severity will be reduced, but we will still have to learn to live with the virus for the foreseeable future.
To debunk myths and manage expectations around the vaccine, Investec Life invited Professor Francois Venter, one of South Africa’s foremost experts on the virus, to share his insights on a webcast. A Professor of Medicine at Wits University, Francois is also a leading light in the fight against HIV/Aids.
Joining Francois in the conversation, moderated by Kalay Maistry, is Sinenhlanhla Sithomo, Head of Insurance Business at Investec Life, who offered his views on how the vaccine could impact life insurance and the "uncertainty mindset" the pandemic has helped us adopt.
When will things return to normal?
We should probably accept that we’ll all contract the virus at some point – it’s simply too infectious and too pervasive to avoid completely. The key is getting over the immune system bombardment of the first infection; each subsequent infection after that will likely be easier for the body to overcome. And this is precisely how we’ll deal with Covid in the future – by learning to live with it.
But how soon with things normalise? Francois gives three scenarios on how the virus will play out:
The best-case scenario, that the scientific community strongly predicts is the most likely, is the "common cold scenario", where you will occasionally get the virus and your body will learn to fend it off like the common cold. "There’ll be Covid circulating in the air and on surfaces, but it won’t be life threatening," explains Francois. In this case, things could return to normal sooner rather than later.
The second scenario is less than ideal and will occur if Covid-19 immunity wanes quicker than we think. This would mean that you'd need to get an updated vaccine every three to five years, and drug researchers would need to stay one step ahead of the virus.
Finally, there’s the worst-case “Armageddon” scenario, where the virus becomes so mutagenic that most people will require a new vaccine each year to avoid getting too sick. The most vulnerable among us – like the elderly and diabetics – will live in continual fear of getting infected and face masks and social distancing will stay with us indefinitely.
Prefer to listen on the go?
Listen to the podcast of the discussion between Prof Venter and Sinenhlanhla Nzama.
The "South African variant" is a misnomer
Viruses, Francois notes, have little interest in killing their hosts because this halts transmission. Viruses mutate to become more infectious but less lethal over time, which often happens at a hyper-local level – the “Durban” version may be slightly different to the “Johannesburg” version, the “New York” version and so on.
"There are probably thousands of variants all competing with each other to be the next most effective and fit version that's going to take over," says Francois.
Even then, naming mutations by their location is problematic: the place where a mutation occurs and the place where it’s picked may be different; it also wrongly inculcates the kind of irrational prejudice that continues to drive Sinophobia and finger pointing in many parts of the world.
Herd immunity unlikely
Of all the epidemiological jargon that has become part of our daily vocabulary – none has captured our imagination more than the term “herd immunity”. Some scientific models say that up to 65% of a population must be vaccinated in order to reach this Holy Grail of virology. Francois believes it’s an unattainable goal…
“There will be no herd immunity, there will be just a circulating virus going round and round that we'll all get every couple of months,” explains Prof Venter.
So, the goal isn’t herd immunity but rather individual immunity. Much like the flu, this means acquiring the ability to cope with the range of illnesses caused by Covid-19 rather trying to eradicate the virus completely.
This is particularly important for those with high-risk comorbidities like diabetes. Current clinical reports show that diabetics with Covid-19 are twice as likely to need intensive hospitalisation.
“The vaccines are not going to give you sterilising immunity, they’re not going to protect you absolutely from infection, but they are going to stop all the horrible things that can happen,” says Francois, like hospitalisation, sever illness and long Covid.
The rise of vaccine nationalism
Globally, we know that vaccine manufacturing capabilities have been heavily stress-tested and deliveries have been delayed. Even as countries like the US and UK have begun making good strides in their programmes, vaccinating the whole world is a logistical challenge, and worldwide distribution remains uneven and split across the lines of wealth and influence.
The rise of vaccine nationalism, where some countries buy-up and hoard more vaccines than they require, is ugly but "depressingly predictable", says Francois, and until that self-corrects we should continue to maintain physical distancing and wear masks as we always have since the pandemic started.
With first world countries moving quickly towards vaccinating 90%–100% of their populations, and third world countries still at less than ten percent, it raises an ethical dilemma, says Sinenhlanhla. "You still have the elderly and people with chronic conditions who are actually last in line compared to someone who stays in a first world country who's 20 and has got a fighting chance against the virus.”
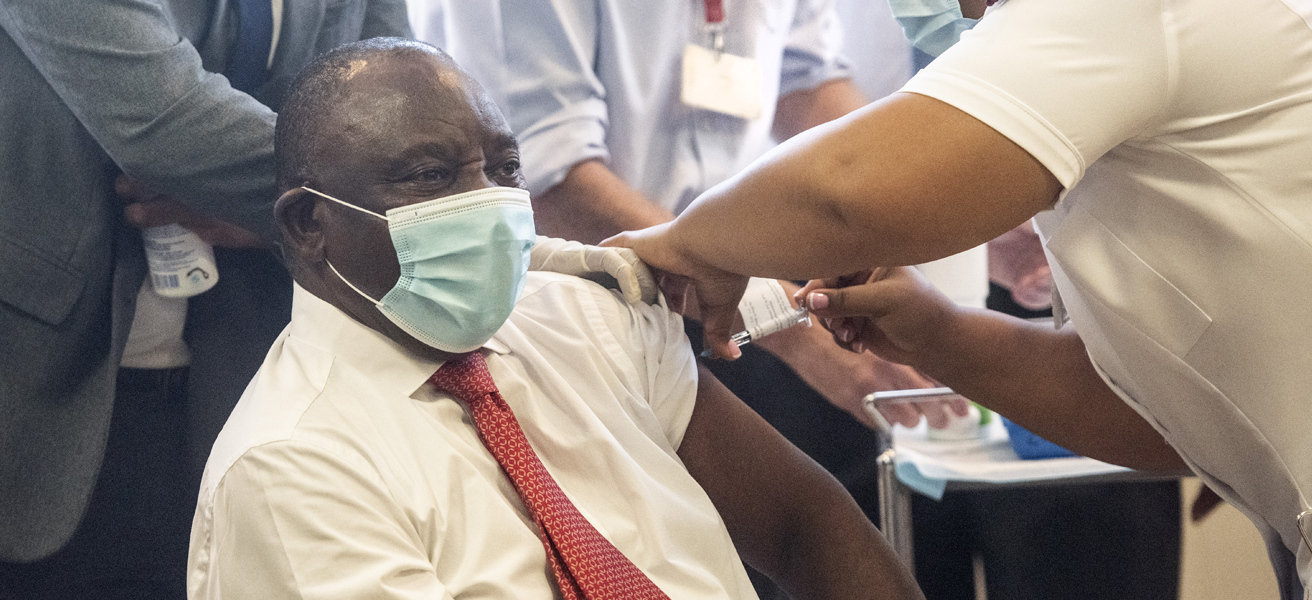
President Cyril Ramaphosa receiving his Covid-19 jab on 17 February 2021 at the Khayelitsha District Hospital in Cape Town.
How vaccines might impact your insurance cover
If we extend this idea of a green passport into the insurance sector, will there ever be a time that you will have to be vaccinated against Covid-19 or risk not getting cover?
“It’s still uncertain. One thing with insurance is that we deal very well with risk where you know the possible outcomes and the probability of those outcomes. Here we know the possible outcomes but not much about the probabilities, that's why it's uncertain,” says Sinenhlanhla.
These probabilities include the possibility that even if you don't have the vaccine, you will be protected because of a strong population immunity.
“But the question for us as an insurer to consider is will there be any substantial risk differential between those who are vaccinated and those who are not? Does this risk differential change for future strains or variants of the coronavirus?” Not to mention the mystery surrounding long Covid and the potential impact to insurers down the line.
If it does become possible to quantify the risk, then antivaxxers may face increased premiums – a principle that’s universally well accepted in risk underwriting for everything from heart conditions to smoking, says Sinenhlanhla.

Lockdown South Africa: one year on
One year since South Africa went into lockdown, Professor Glenda Gray, a leader in the fight against Covid-19, reflects on wins, losses, lessons learnt and the vaccination challenge.
Lessons learned from the HIV/Aids crisis
Just like the vaccine hesitancy we are seeing across South Africa, people were also afraid to take ARVs when they became available, says Francois. "We had people just would rather die than swallow the tablets.” The way to encourage community buy-in, he says, is by investing in patient education.
Another lesson we've learned from the HIV Aids is that that health is actually a moral imperative. “I think too often over the last 20 to 30 years, it's been kind of the economy is the most important thing, I think we've seen now the economy is actually at the mercy of populations being healthy.”
One of the biggest lessons we've learnt from the current crisis is that it's given us a better understanding of how to deal with uncertainty. "We’re living in a very volatile and uncertain world and I think as we evolve as societies, some of the key lessons we’re learning from this virus is how do you respond to such uncertainty especially if it's so widespread,” says Sinenhlanhla. The answer, he says, is closer collaboration between government, business and Individuals.
Prof Francois Venter bio
Francois is a Medical Professor at Wits University and has been on the frontline of Covid-19 research in South Africa. He was among the first in South Africa to volunteer for a Covid-19 vaccine trial in late 2020.
Francois is Director of Ezintsha, a group of South African academic and health professionals who looks for ways to apply new technology to health-related problems, and to extend access to effective drugs to everyone. Ezintsha is part of the Wits Reproductive Health and HIV Institute.
Notable achievements
- Honorary consultant at Charlotte Maxeke Johannesburg Academic Hospital
- Previous president of the SA HIV Clinicians Society
- Pioneering work in HIV programme implementation and ART in South Africa
About the author

Ingrid Booth
Lead digital content producer
Ingrid Booth is a consumer magazine journalist who made the successful transition to corporate PR and back into digital publishing. As part of Investec's Brand Centre digital content team, her role entails coordinating and producing multi-media content from across the Group for Investec's publishing platform, Focus.
Get in touch
If you have any feedback or suggestions, please let us know
You may also be interested in:

Severe Illness Cover

Life Cover

Mortgage Protection Cover
Severe Illness Cover
Life Cover
Mortgage Protection Cover
Browse further in